

Folic acid versus folate. Which one is the best supplement for family planning and supporting a healthy pregnancy?
There’s a lot of speculation as to whether we’re likely to see a post-pandemic baby boom. Want-to-be parents and expectant mothers may be busy researching and reviewing the importance of folic acid in terms of preconception and prenatal health. Nutritional Therapist Jackie Newson reveals why folate supplements win the debate…
Good nutrition
To cover all bases, a well-balanced diet including regular intake of omega 3 fats, good quality protein and generous portions of fruit and vegetables is a must during pregnancy. In addition to this, it’s recommended that all mums-to-be supplement their diet with 400mcg of folic acid per day – or should it be folate? A good question that may leave some mums-to-be a little confused.
What is the difference between folic acid and folate?
Both folic acid and folate are forms of vitamin B9 and although people frequently use both names interchangeably there are in fact some important differences between the two. Folate is the naturally occurring and active form of vitamin B9, whereas folic acid is the synthetic form often used in supplements.
Folic acid is commonly used to fortify foods such as bread, pasta, rice and breakfast cereals. This synthetic version is incorporated into fortified foods because it is known to be more heat-stable than the folate found naturally in many foods5.
How to make sure you’re getting active folate into your cells
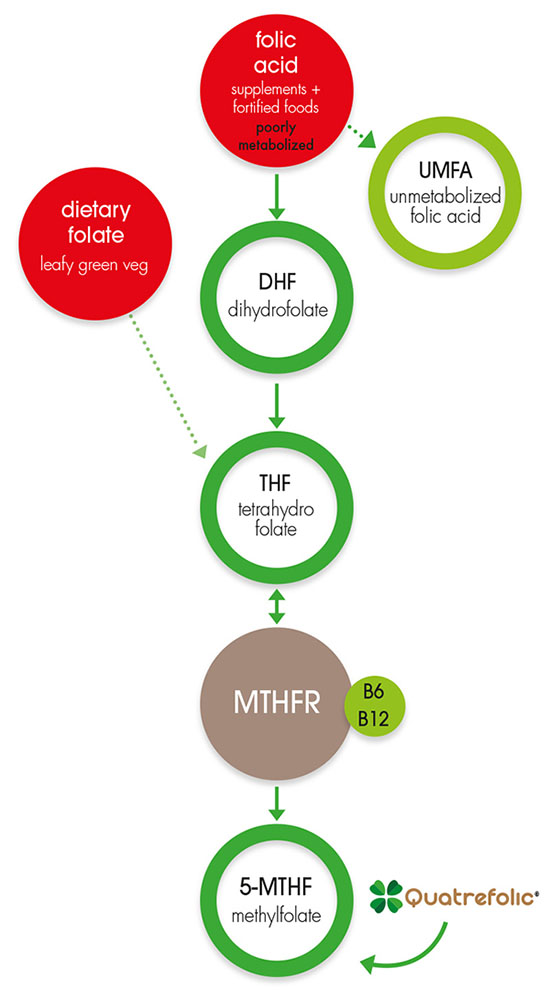
Folate is a water-soluble compound which the body is unable to make and must, therefore, obtain from dietary sources. The body converts folate into the metabolically active form of folate called 5-methyltetrahydrofolate (5-MTFH), which is readily utilised by the cells.
Cooking destroys folate levels
Most naturally occurring food sources of folate are already in this active form, however cooking and processing destroys these folate compounds.
Cells require the active form of folate
The process of converting folate into the metabolically active form is relatively complex and requires several enzymes including methylenetetrahydrofolate reductase (MTHFR). To aid this metabolic process, the body needs good intestinal and liver function, as well as a sufficient supply of vitamins C, B2, B3, B6, the mineral zinc and an amino acid called serine14.
Could you be missing the activation enzyme?
Despite this complicated process, evidence suggests that folic acid supplementation increases body stores of 5-MTHF in healthy people12. However, this isn’t the case for people who lack the MTHFR enzyme needed to convert folic acid to 5-MTHF. For those with this folate metabolism disorder, supplementing with 5-MTHF is recommended as it is seen to be more beneficial than folic acid supplements14.
Is Quatrefolic® the best folate supplement?
Quatrefolic is a glucosamine salt formed by combining the active form of folate 5-MTHF with glucosamine. This form of folate has long-lasting stability, high water solubility and well-established safety. Studies suggest that Quatrefolic has an important advantage over synthetic folic acid because it is well absorbed even when pH in the gut is altered.
An increasing body of evidence reports the advantages of using active folate supplements such as Quatrefolic. Previously, a calcium salt of 5-MTHF was available in supplement form but it quickly became evident that this form had limitations related to stability and poor solubility.
In America, around 25% of Hispanics and 10-15% of Caucasians and Asians have two genetic mutations in the MTHFR gene11. This genetic abnormality inhibits their ability to convert folic acid into the active form by approximately 70%. Methylfolate supplements are usually recommended to people with this genetic mutation. By supplementing with 5-MTHF you are cleverly bypassing the mutated MTHFR and providing the body with the already active form of folate which can be easily utilised.
The absorption and uptake of Quatrefolic is not affected by metabolic defects11. What’s more, because it is in the active form, it’s accessible to body cells as soon as it’s absorbed.
The role of folate in the body
The action of folate in the body is similar to vitamin B12. Folate is necessary for the process of cell division and multiplication making it especially important for foetal development and maternal tissue growth during pregnancy.
Essential for a healthy pregnancy
Supplementing in the months before conception and the first trimester of pregnancy is known to significantly reduce the risk of serious birth defects of the central nervous system. It is therefore vital that women planning a pregnancy obtain sufficient dietary levels of folate. Folate also helps with red blood cell formation and aids in the production of RNA and DNA (the carriers of genetic information).
Folate contributes to many other functions including:
- The reduction of tiredness and fatigue
- Normal amino acid synthesis
- Normal blood formation
- Normal homocysteine metabolism
- Normal psychological function
- Normal function of the immune system
Folate and neural tube defects
Neural tube defects are congenital malformations that affect the brain and spinal cord during embryonic development and may result in conditions such as spina bifida and anencephaly. Neural tube defects develop during the very early stages of pregnancy, often before a woman is aware that she is pregnant.
An overwhelming body of evidence links folate deficiency in the early stages of pregnancy to an increased risk of the baby developing neural tube defects7. During the early stages of pregnancy, the neural tube is formed and closes properly within the first weeks of pregnancy, a process that may be helped by consuming folate, before and during early pregnancy5.
Folate, mood and mental health
Folate is known to contribute to normal psychological function, and this may be because it’s involved in the production of key mood uplifting neurotransmitters. Folate is a cofactor for serotonin synthesis10 and studies have shown a link between low folate levels and low mood1. Research has also identified that individuals with MTHFR deficiency tend to produce lower levels of serotonin17.
Folate and healthy homocysteine levels
Folate is known to contribute to normal homocysteine metabolism. It plays a key role in breaking down homocysteine into an essential amino acid called methionine. Without enough folate to facilitate this process, homocysteine may rise to harmful levels. High homocysteine levels have been linked to infertility, recurrent miscarriages and cardiovascular disease 3,13,16.
Food sources of folate
Folate may be easily destroyed during prolonged storage and up to 50% may be lost during cooking6. Good food sources of folate include:
- Green leafy vegetables
- Asparagus
- Bean sprouts
- Wheat germ
- Whole grains
- Oranges
- Berries
- Cantaloupe
- Pineapple
- Bananas
- Seafood
- Beans
- Peanuts
- Sunflower seeds
- Liver
- Eggs
Why folic acid isn’t the best supplement
Folic acid is a synthetic molecule which requires four conversions to produce the active form. It is highly dependent on individual genetics and other nutrients for efficient and effective conversion. As well as this, excessive folic acid supplementation may overwhelm the liver’s ability to metabolise the folic acid, leading to a build-up of un-metabolised folic acid (UMFA).
Consuming food fortified with folic acid together with additional supplementation during pregnancy could easily result in ingesting over the safe upper limit of 1000mcg/day. For example, a bowl of breakfast cereal may have 400mcg of added folic acid2.
The consequences of prolonged exposure to circulating UMFA are largely unknown as this has not been thoroughly investigated. But for the moment there is no conclusive evidence that UMFA causes adverse health effects. However, some experts are still of the opinion that the biological effects of excessive levels of folic acid are not without risk 8,10,15.
Potential risk factors to consider include:
- The body has limited ability to metabolise folic acid especially in high doses
- Several studies suggest that excessive levels of folic acid increase the risk of certain cancers
- Folic acid binds to a gene that affects the ability of those with MTHFR mutations to correct a folate deficiency
- Studies have found that UMFA leads to immune dysfunction. Dysfunctional immune effects have been seen in post-menopausal women who consumed a folate-rich diet together with folic acid supplements of more than 400mcg/day
With regards to supplementation, always look for a nutritional supplement containing a natural form of folate rather than synthetic folic acid, preferably such as Quatrefolic, for a form of folate that’s already been activated and ready for the body to utilise.
Jacqueline Newson BSc (Hons) Nutritional Therapy
REFERENCES
- Bolander-Gouaille C ,Coppen A. Treatment of Depression: Time to Consider Folic Acid and Vitamin B12. J Psychopharmacol. 2005: 19, 1: 59-65.
- DeSoto MC and Wiens D. Is High Folic Acid Intake a Risk Factor for Autism?—A Review. Brain Sc. 2017; 7,11: 149.
- D'Uva M, Di Micco P, Strina I, et al. Hyperhomocysteinemia in women with unexplained sterility or recurrent early pregnancy loss from Southern Italy: a preliminary report. Thromb J. 2007;5:10.
- Fava M & Mischoulon D. Folate in Depression: Efficacy, Safety, Differences in Formulations, and Clinical Issues. The Journal of clinical psychiatry 2009;70, 5: 12-7.
- https://www.cdc.gov/ncbddd/folicacid/faqs/faqs-general-info.html. [Accessed 9.6.20.]
- https://www.sciencedirect.com/topics/chemistry/folic-acid. [accessed 9.6.20]
- herrmann M, Kasoha M, Kirsch SH & Obeid R. Concentrations of unmetabolized folic acid and primary folate forms in pregnant women at delivery and in umbilibal cord blood. AJCN. 2010; 92:1287-88.
- Koren G, O’Connor D and Tam C. Circulating Unmetabolized Folic Acid: Relationship to Folate Status and Effect of Supplementation. Obstetrics and Gynecology Interantional 2012; 485179: 1-17.
- Lamers Y, Prinz-Langenohl R, Bramswig S,Pietrzik K. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. Am J Clin Nutr. 2006;84:156-161.
- MTHFRSUPPORT Australia. Should you supplement with Folic Acid or Active Folate (5-MTHF)? https://mthfrsupport.com.au/2015/05/folic-acid-vs-5-mthf-treating-mthfr-deficiency/. [Accessed 11.6.20]
- Panzavolta G, Scaglione F. Folate, Folic Acid and 5-methyltetrahydrofolate Are Not the Same Thing. Xenobiotica. 2014;44(5):480-8.
- Priest DG, Schmitz JC, Bunni MA. Accumulation of plasma reduced folates after folic acid administration. Semin Oncol 1999;26:S38-S41.
- Refsum H, Ueland PM, Nygard O, Vollset SE. Homocysteine and cardiovascular disease. Annu Rev Med. 1998; 49: 31–62
- Thorne Research. 5-Methyltetrahydrofolate monograph. Alternative Medicien Review 2006; 11,4: 330-337.
- Ware WR. Raising Concerns About Unmetabolized Folic Acid. Journal ofOrthomolecular Medicine 2008; 23,1: 43-51.
- Wilcken DE, Wilcken B. The pathogenesis of coronary artery disease. A possible role for methionine metabolism. J Clin Invest. 1976; 57: 1079–108
- Young SN. Folate and depression--a neglected problem. J Psychiatry Neurosci. 2007;32(2):80‐82.
Related posts
-
.jpg?auto=format&q=45&w=262&trim=auto) Unlocking Fertility: The Critical Role of B Vitamins for Men and WomenWhile assisted reproductive technologies offer valuable support for couples struggling to conceive, research...
Unlocking Fertility: The Critical Role of B Vitamins for Men and WomenWhile assisted reproductive technologies offer valuable support for couples struggling to conceive, research... -
.jpg?auto=format&q=45&w=262&trim=auto) BEST FOODS FOR MARATHON RUNNERS: PRE-RACE FUEL & POST-RUN RECOVERYMarathon day is approaching, and if you’re one of those fitness enthusiasts hoping to cross the finish line in good...
BEST FOODS FOR MARATHON RUNNERS: PRE-RACE FUEL & POST-RUN RECOVERYMarathon day is approaching, and if you’re one of those fitness enthusiasts hoping to cross the finish line in good... -
 Celebrating Vitamin C During Hay Fever SeasonSpring in all its glory with blossoming trees on every corner, really is a ‘sight for sore eyes’, especially for...
Celebrating Vitamin C During Hay Fever SeasonSpring in all its glory with blossoming trees on every corner, really is a ‘sight for sore eyes’, especially for...